Our planned pilot of the SCOREIT motor developmental screener (funded by NICHD SBIR Grant HD095783) was launched earlier this year at the Kindering clinic (Bellevue, WA). SCOREIT will run as a screening tool in the pediatrician’s office, a community health center near you, or a similar venue. Post-covid, we expect these sessions to be administered either via Zoom or in-person, as appropriate. We have conducted five day-long sessions and evaluated 28 infants thus far in this pilot program.
The primary purposes of the SCOREIT Pilot are to conduct motor screening in a clinical setting, understand the physical, technical, workflow, and staffing requirements of SCOREIT, drive development of the SCOREIT webapp tool through feedback from clinicians, and specification of detailed processes that describe conduct of the motor screening in a controlled clinical setting and later evaluation of the infant’s motor development through retrospective, asynchronous review of the observation videos. Additionally, the pilot will also yield rich motor development data from 40 infants, which will be used to further the automation goals of SCOREIT.
Facility Requirements. We drew from a wealth of experience conducting the Phase I study of SCOREIT over the past three years. The Phase I study allowed us to specify minimum requirements in terms of physical space, access, equipment, personnel, and technology. We used the pilot to refine these requirements to suit the clinical environment and workflow.
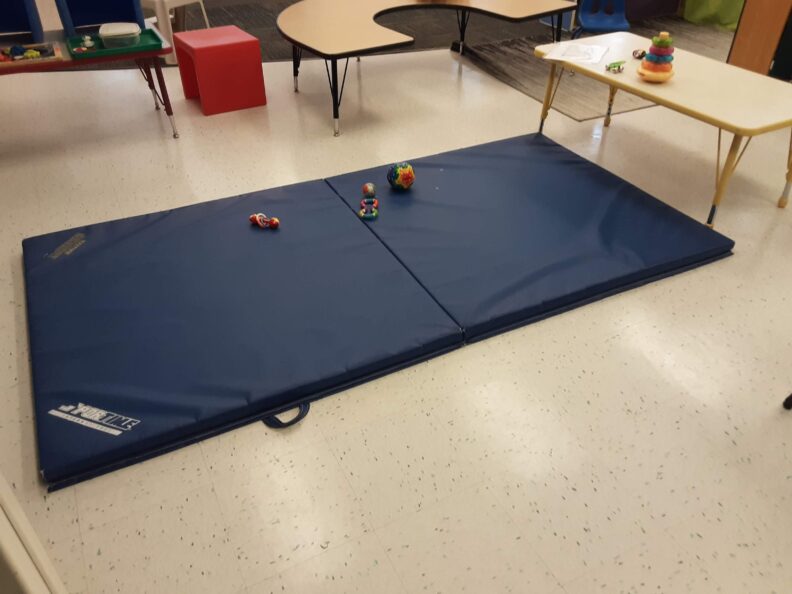
SCOREIT has pretty minimal facility requirements. Kindering had space, for sure. All they needed to do was repurpose a gym mat and move some furniture pieces around. Parents usually bring their infants’ favorite toys, but it is supplemented by what Kindering already had in their clinic.
Technology requirement is minimal as well. We used an off-the-shelf Android tablet with wifi connection. The tablet, shown above, is mounted on a tripod with a ballhead for easy manipulation of camera angle.
Motor Screening in the Clinic. We are using the pilot to develop detailed yet succinct protocols to guide the parent as they engage in play activities with their infant at the clinic (in front of the camera). Administration of the Alberta Infant Motor Scale (AIMS) requires minimal adult assistance in eliciting infant movement. Guidance by the clinician (e.g., occupational therapist) is in the form of cues to the parent to elicit infant movement and positioning of the infant (and the parent) to promote parent-child interaction and child comfort.
The current practice is to prepare the parent with materials that consist of static figures and checklists. We are finding this an onerous requirement. So, instead, we are developing short videos that the parent views prior to the clinic appointment. This knowledge is then complemented by appropriate realtime cues from the clinician based on the posture of the infant (i.e., if the infant is supine, prone, sitting, or standing) and the developmental stage of the infant (i.e., if the infant is not yet rolling over, is rolling over and beginning to move, or is sitting and might walk).

SCOREIT Webapp Tool. SCOREIT is a telehealth technology solution for early motor screening. It will support acquisition of observation videos from play activities, management of observation data in the cloud, asynchronous evaluation of observation data from videos, scoring of motor development from tagged motor items in the videos, and creation and delivery of the motor evaluation report to the parent.
We are using the pilot to obtain clinician feedback and integrate the app workflow into the clinical environment. Significant improvements have been made to all aspects of the app as we move from the ‘lab’ to the ‘marketplace.’
The SCOREIT webapp has been enhanced in the following areas of functionality:
- Video Acquisition. We began the pilot program with the assumption that a platform like Zoom can be used to record the infant observation sessions and add the saved recordings to SCOREIT prior to video tagging and motor evaluation. It became clear immediately that reliance on 3rd party software would lead to integration and customer adoption barriers as well as introduce opportunities for errors, where a video belonging to one subject could be mistakenly uploaded to a different subject.
We were able to quickly add an in-app video recording option that allows the therapist to pull up a subject’s information and record the ensuing observation session. This functionality eases conduct of the assessment session and prevents errors.


- Report Generation. A considerable amount of time and effort were being expended in producing the motor evaluation reports. Additionally, the process was replete with opportunities for error, especially in mis-identifying records belonging to different subjects or the incorrect report being sent to a parent.
Feedback from the pilot has allowed us to build out a more comprehensive, integrated reporting functionality into the SCOREIT webapp. THis will allow the therapist to prepare a PDF report for a motor assessment session at the touch of a button. Additional functionality has also been built to communicate, via email, the evaluation report with the parent.
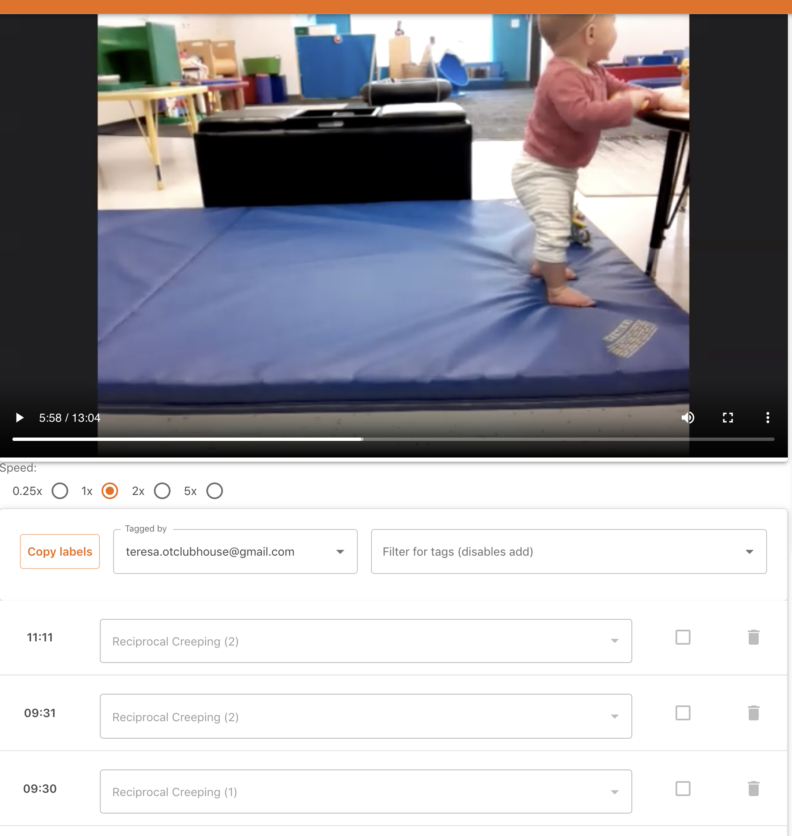
- Video Tagging. SCOREIT allows a remote developmental expert to access video recordings of infant motor assessment sessions and tag/label them with motor items from an evaluation instrument such as AIMS. That this process can be executed asynchronously from the administration at a clinic can lead to efficiencies, remote accessibility of expertise, and cost savings.
We were able to observe the app’s usage among the multiple participants in the pilot program. We introduced several features, unplanned at the start of the pilot, in order to make the process of video tagging more efficient. These included automatic saving of labels, speed controls for the video player to allow fine-grained inspection, keyboard controls for oft-repeated tasks, multiple label sets to allow multiple users to tag videos, review options that allow a therapist scoring a video to request additional review of specific motor items, automated scoring from manually marked motor item labels, automated look-up of percentile scores, and automated generation of motor evaluation reports, to name a few.