Our patent just issued: US Patent No. 12,272,054, protecting the core technology behind Cribsy — our AI-powered platform for early identification of neuromotor risks in infants using home-recorded video.
This patent secures not just our approach to risk detection, but also Cribsy’s ability to track developmental progress and support timely interventions. In short, it protects the full arc of what makes Cribsy unique:
-> from observation to insight to impact.
As we prepare for broader adoption in pediatric care, this milestone helps ensure Cribsy remains a trusted and scalable tool for early detection and monitoring.
To the families who have shared their time and videos, and to our funders at NIH/NICHD through the SBIR program—thank you for making this work possible.
Our early developmental screener for infants, Cribsy, has been awarded a prestigious Phase I SBIR (Small Business Innovation Research) grant from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD) 🎉
In underserved and rural communities, the need for early developmental screening and early intervention is pressing. Our goal is to develop Cribsy into a scalable AI system that can be widely adopted, ensuring that minority populations are adequately represented and racial/cultural biases in AI systems are addressed.
This Phase I funding will allow us to refine Cribsy, making it more efficient, stable, scalable, and cost-effective. We are excited to take this significant step towards improving early developmental screenings and making a positive impact on infant health.
Stay tuned for more updates as we advance this groundbreaking project! 🚀
Cribsy is an innovative smartphone-based telehealth screener designed to identify neuromotor risks in infants. This user-friendly, automated tool aims to address a critical need: early diagnosis and intervention for developmental disabilities, which affects 5-10% of children in the US.
We had a series of chats with Early Markers chief clinical officer, Dr. Teresa Fair-Field on infant development and screening for delays and disorders. In this snippet, Dr. Fair-Field explains why we should screen infants at home.
We started with a simple but ambitious hypothesis: we can automate developmental assessment of an infant from passive observational data (video) of infant movements. We just have to figure out where the infant is in the video (pose estimation) and then what kind of movements are transpiring (activity classification). Finally, we use a clinically validated assessment tool and the extracted activities from video to decide if the infant is developing typically or if they need follow-ups. Simple, right?
We have completed several studies in which we gathered high-quality infant movement data and built Machine Learning (ML) engines to determine infant pose and perform motor activity classification. Our recent publication (see below) focuses on an essential problem that could thwart automated extraction of infant development metrics. A clinically validated assessment protocol such as the Alberta Infant Motor Scale (AIMS) has 58 motor items that an expert assessor looks for in the process of evaluating a child. FIFTY EIGHT! That’s a whole lot to automate. A state of the art human activity classification engine typically might handle less than twenty. So, the question is: are all 58 items important? Can we use 20? 15? If yes, then which ones?
The good news is, you can make do with an abridged assessment tool that does not require 58 items. Using far fewer items can still produce valid results in assessing an infant. Fewer items means shorter time to evaluate the infant. And, best of all, easier to build a fully automated ML system that can analyze home videos and screen for developmental delays.
Check out our recent article on Elsevier’s journal of Early Human Development.
Virtual student research opportunities are continuing here at Early Markers! We are hosting three new occupational therapy students- Kiana A., Sheri K., and Ginny K. from Pacific University. The doctoral students are completing their capstones with us via Zoom and Slack to assist with our current infant studies.
Sheri’s capstone project focused on studying the efficiency in administration and inter-rater reliability of the Alberta Infant Motor Scale [AIMS] salient-set screening tool. This research will support Early Makers in the development of an efficient and reliable automated screening tool for the detection of motor delay in the first year infant.
Kiana’s capstone focused on collecting pre-pilot customer discovery insights from a questionnaire and two focus groups. The goal is to understand the experience of preterm infant parents; specifically their concerns, access to resources, experience with current health care services, and response to the EMMA app concept (now available on Google Play and the Apple app store).
The outcome of Ginny’s capstone is the study and creation of content for the EMMA app’s library of Parent Activity Modules (PAM). The PAM library will provide educational resources to parents in an accessible format to promote developmental milestones in infants using a parent-led, play-based intervention approach.
All three graduate students have found this to be a great opportunity to learn about infant development, clinical research, the administration of infant motor development assessments, and the creation of family-centered media content. Watch for their OTD capstones to be presented in poster sessions at the American Occupational Therapy Association [AOTA] conference, Inspire 2023 in Kansas City, MO.
The experience has overall been wonderful for both our Early Markers team and students alike. We are excited to see how their research questions of interest take shape and help us in creating content for our EMMA app!
Our planned pilot of the SCOREIT motor developmental screener (funded by NICHD SBIR Grant HD095783) was launched earlier this year at the Kindering clinic (Bellevue, WA). SCOREIT will run as a screening tool in the pediatrician’s office, a community health center near you, or a similar venue. Post-covid, we expect these sessions to be administered either via Zoom or in-person, as appropriate. We have conducted five day-long sessions and evaluated 28 infants thus far in this pilot program.
The primary purposes of the SCOREIT Pilot are to conduct motor screening in a clinical setting, understand the physical, technical, workflow, and staffing requirements of SCOREIT, drive development of the SCOREIT webapp tool through feedback from clinicians, and specification of detailed processes that describe conduct of the motor screening in a controlled clinical setting and later evaluation of the infant’s motor development through retrospective, asynchronous review of the observation videos. Additionally, the pilot will also yield rich motor development data from 40 infants, which will be used to further the automation goals of SCOREIT.
Facility Requirements. We drew from a wealth of experience conducting the Phase I study of SCOREIT over the past three years. The Phase I study allowed us to specify minimum requirements in terms of physical space, access, equipment, personnel, and technology. We used the pilot to refine these requirements to suit the clinical environment and workflow.
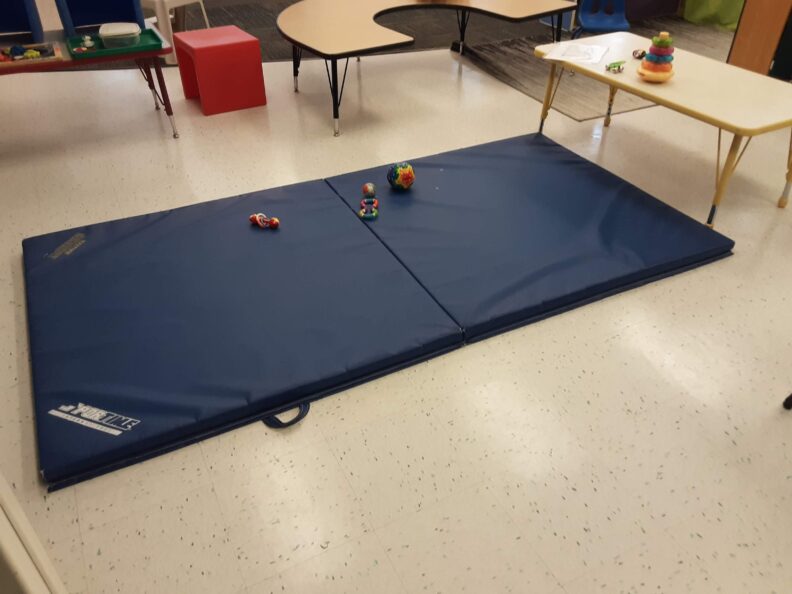
SCOREIT has pretty minimal facility requirements. Kindering had space, for sure. All they needed to do was repurpose a gym mat and move some furniture pieces around. Parents usually bring their infants’ favorite toys, but it is supplemented by what Kindering already had in their clinic.
Technology requirement is minimal as well. We used an off-the-shelf Android tablet with wifi connection. The tablet, shown above, is mounted on a tripod with a ballhead for easy manipulation of camera angle.
Floor play setup. Equipment and space requirements for administration of Alberta Infant Motor Scale (AIMS) are minimal.
Motor Screening in the Clinic. We are using the pilot to develop detailed yet succinct protocols to guide the parent as they engage in play activities with their infant at the clinic (in front of the camera). Administration of the Alberta Infant Motor Scale (AIMS) requires minimal adult assistance in eliciting infant movement. Guidance by the clinician (e.g., occupational therapist) is in the form of cues to the parent to elicit infant movement and positioning of the infant (and the parent) to promote parent-child interaction and child comfort.
The current practice is to prepare the parent with materials that consist of static figures and checklists. We are finding this an onerous requirement. So, instead, we are developing short videos that the parent views prior to the clinic appointment. This knowledge is then complemented by appropriate realtime cues from the clinician based on the posture of the infant (i.e., if the infant is supine, prone, sitting, or standing) and the developmental stage of the infant (i.e., if the infant is not yet rolling over, is rolling over and beginning to move, or is sitting and might walk).
We started out the pilot recording observation sessions via a tripod mounted Android tablet via Zoom.
SCOREIT Webapp Tool. SCOREIT is a telehealth technology solution for early motor screening. It will support acquisition of observation videos from play activities, management of observation data in the cloud, asynchronous evaluation of observation data from videos, scoring of motor development from tagged motor items in the videos, and creation and delivery of the motor evaluation report to the parent.
We are using the pilot to obtain clinician feedback and integrate the app workflow into the clinical environment. Significant improvements have been made to all aspects of the app as we move from the ‘lab’ to the ‘marketplace.’
The SCOREIT webapp has been enhanced in the following areas of functionality:
Video Acquisition. We began the pilot program with the assumption that a platform like Zoom can be used to record the infant observation sessions and add the saved recordings to SCOREIT prior to video tagging and motor evaluation. It became clear immediately that reliance on 3rd party software would lead to integration and customer adoption barriers as well as introduce opportunities for errors, where a video belonging to one subject could be mistakenly uploaded to a different subject.
We were able to quickly add an in-app video recording option that allows the therapist to pull up a subject’s information and record the ensuing observation session. This functionality eases conduct of the assessment session and prevents errors.
Video recording is now integrated into the SCOREIT app. In addition to the convenience factor, integrated video recording also prevents errors.Parents watch a 3-min video on how to conduct the play activities. They need occasional prompting from the ‘remote’ therapist on how to position themselves and the baby. Additional prompting were required to elicit activities from the infant.
Report Generation. A considerable amount of time and effort were being expended in producing the motor evaluation reports. Additionally, the process was replete with opportunities for error, especially in mis-identifying records belonging to different subjects or the incorrect report being sent to a parent.
Feedback from the pilot has allowed us to build out a more comprehensive, integrated reporting functionality into the SCOREIT webapp. THis will allow the therapist to prepare a PDF report for a motor assessment session at the touch of a button. Additional functionality has also been built to communicate, via email, the evaluation report with the parent.
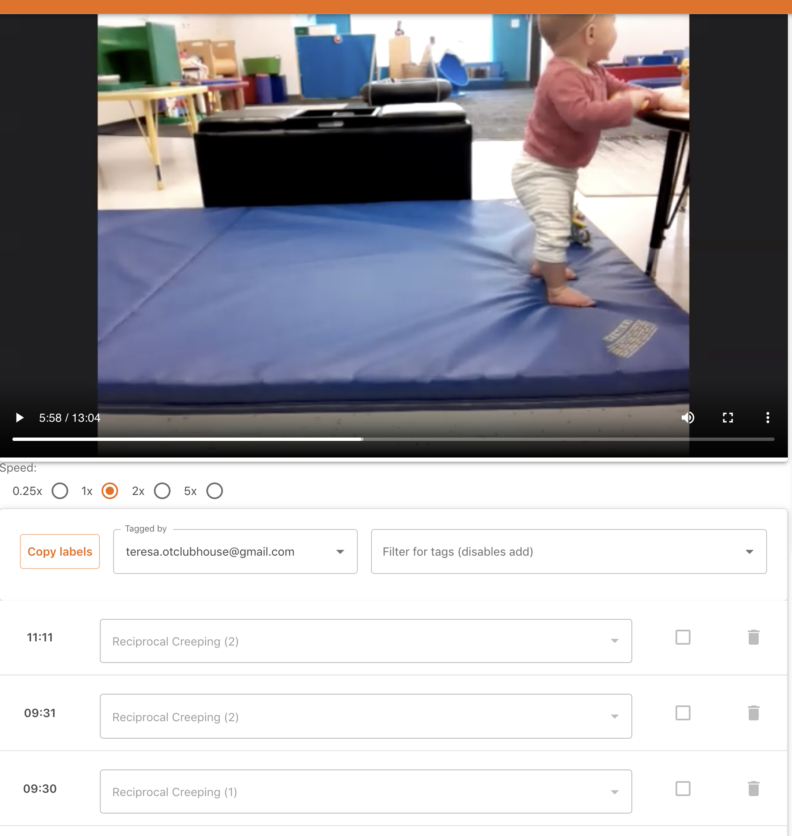
Video Tagging. SCOREIT allows a remote developmental expert to access video recordings of infant motor assessment sessions and tag/label them with motor items from an evaluation instrument such as AIMS. That this process can be executed asynchronously from the administration at a clinic can lead to efficiencies, remote accessibility of expertise, and cost savings.
We were able to observe the app’s usage among the multiple participants in the pilot program. We introduced several features, unplanned at the start of the pilot, in order to make the process of video tagging more efficient. These included automatic saving of labels, speed controls for the video player to allow fine-grained inspection, keyboard controls for oft-repeated tasks, multiple label sets to allow multiple users to tag videos, review options that allow a therapist scoring a video to request additional review of specific motor items, automated scoring from manually marked motor item labels, automated look-up of percentile scores, and automated generation of motor evaluation reports, to name a few.
Video tagging of motor activities can be done asynchronously and remotely using the SCOREIT web app.
Kindering therapists tried out ‘live’ scoring of the infant. They much prefer asynchronous scoring of the observation sessions using the SCOREIT tool.The sterling crew has completed 28 infant sessions so far, spread over five day-long sessions.
We are building a library of parent activity videos to assist parents with play-based activities that can augment their child’s development and enhance parent-child bond. These play-based activities will be delivered as part of the EMMA app that is currently under development.
Late 2019, we held a day-long photo shoot session at Early Markers facilities to gather play-based activities data from eight infants between 3-6 months. We have been developing short videos, Motor Minutes, that target developmental milestones for this age group. Look below for a sample video that targets prone tolerance (‘tummy time’).
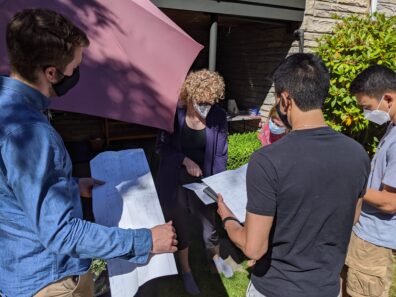
The pandemic interrupted our plans to gather data from infants in the 6- and 9-month age groups. In August 2020, we were able to kick off another data gathering session. This time, the session would take place outdoors. Aside from the pediatric occupational therapist, Dr. Fair-Field, others would be socially distanced. Dr. Fair-Field wore proper PPE. Two subjects participated in the photo shoot session. Both were healthcare professionals that understood that the risks were minimal. In the words of one of the parents ‘research needs to proceed!’
Now, we are ready to create additional play activity videos for the 6-month age group. Our deep gratitude to the participating parents.
We hosted three WSU School of Medicine students — Jae C, Nick C, and Adam K, as part of the Summer Research Opportunity program. It was a perfect fit for the pandemic summer and a fantastic experience for both the interns and the Early Markers team. We adapted our ongoing infant studies (EMMA and MIMM) to go fully virtual and also conducted all our summer internship activities via Zoom and Slack.
The interns got an immersive education in infant development, clinical administration and assessment of infant motor development using standardized tools, and video coding of motor movements. During the internship, they also got valuable exposure to evaluation of motor skills in the typically developing infant as well as identification of atypical behaviors.
In their final week, they got to observe a ‘live’ motor assessment session (socially distanced), conducted safely outdoors by a pediatric occupational therapist. Their assessments, needless to say, were in excellent agreement with the pediatric OT.
Jae C and Adam K have decided to pursue research questions raised by their involvement with EMMA as part of their longitudinal scholarly project requirements. We are excited to help them explore additional points of scientific validity of EMMA solutions for early developmental screening and home-based, parent-led interventions.

 ur early developmental screener for infants, Cribsy, has been awarded a prestigious Phase I SBIR (Small Business Innovation Research) grant from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD) 🎉
ur early developmental screener for infants, Cribsy, has been awarded a prestigious Phase I SBIR (Small Business Innovation Research) grant from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHD) 🎉